Genomics: Insight
Predictive Role of Succinate Dehydrogenase Mutations and Environmental Factors in Clear-Cell Renal Cell Carcinoma and Pheochromocytomas/Paragangliomas
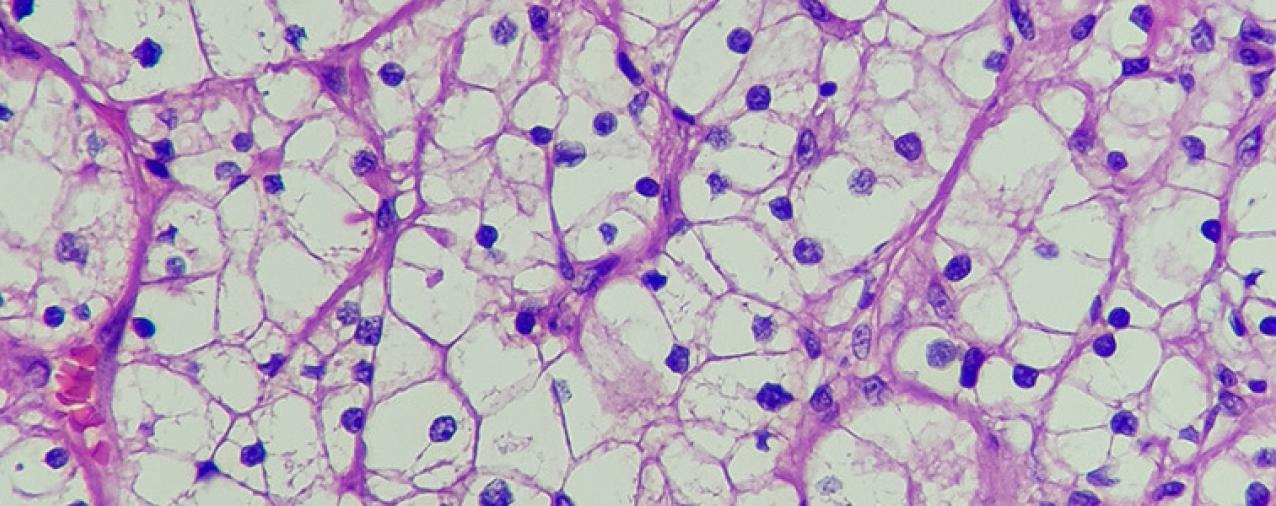
Clear-Cell Renal Cell Carcinoma and Paragangliomas/Pheochromocytomas:
Clear-Cell Renal Cell Carcinoma (ccRCC) accounts for the vast majority (85%) of all renal cancers, with around 64,000 cases reported per year in the United States. Approximately two times more men than women suffer from ccRCC, and it is the 7th most common cancer in men. Patient survival is on average 13 months, with a five-year survival rate under 10% (Skinner et. al., 1971).
Paragangliomas and pheochromocytomas (collectively PPGLs) are rare tumors of the adrenal glands and paraganglia tissue. It has an incidence of 0.58/100,000 per year (Subhi et. al., 2022), occurring most commonly in people aged 30-50. The disease is three times more common in women than in men (Agyun et. al., 2020).
Succinate Dehydrogenase:
In recent years, there has been increasing attention placed on the role of succinate dehydrogenase mutations in cancer development and progression. The succinate dehydrogenase enzyme complex (SDH), also known as respiratory complex II, is an enzyme complex involved in both the Krebs cycle and the electron transport chain. It is implicated in both clear-cell renal cell carcinoma and paraganglioma/ pheochromocytoma.
In paragangliomas and pheochromocytomas, succinate dehydrogenase loss often occurs as a two-hit phenomenon, in which one copy is deleted or inactivated due to germline mutations, and the remaining copy is deactivated by somatic mutation (Prasad et. al., 2009).
SDH and ccRCC:
Until recently, little attention has been paid to the role of SDH in ccRCC. SDH-deficient ccRCC was only recognized by the World Health Organization in 2016 and was considered to make up only 0.05-05% of cases. However, SDH deficiency is increasingly recognized as a common feature of ccRCC. In a 2021 study involving analysis of ccRCC TCGA database data, ccRCC cell lines grown in vitro, and ccRCC samples collected at the Montefiore Medical Center from 2016 to 2019, Aggarwal et. al. showed that SDHB, SDHC, and SDHD were significantly downregulated in ccRCC tumors compared to normal kidney cells (P<0.001). Out of 30 tumors selected for protein expression level evaluation, only two did not exhibit SDHB or SDHD underexpression. Furthermore, patients with SDHB, SDHC, and SDHD down regulation had a significantly lower survival rate, both overall and disease-free.
SDHB, SDHC, and SDHD were significantly downregulated in ccRCC tumors compared to normal kidney cells
In concordance with these findings, a 2022 analysis of the TIMER2 cancer genome database by Yang et. al. showed that low SDHB, SDHC, and SDHD transcription levels had lower disease-free survival rates (P<0.01), and that SDH gene underexpression was correlated with advanced disease progression (P<0.05). 2.2% of patients had SDH mutations, which was correlated with a lower overall survival rate when compared to patients without SDH mutations (P=8.279e-6). Furthermore, ccRCC cells had greatly increased SDHB methylation levels when compared to healthy cells (P<0.001). Methylation refers to the addition of methyl groups to DNA bases, and is generally associated with lower gene expression rates (Moore et. al., 2012). Therefore, ccRCC cells can be reasonably expected to express SDHB at lower levels than healthy cells.
Environmental factors and ccRCC:
There are three primary risk factors for ccRCC: cigarette use, obesity, and hypertension. In 2000, Sweeney et. al. showed that current smokers were approximately 1.7 times as likely as non-smokers to die (95% CI = 1.2-2.5). Furthermore, in a 2005 meta-analysis of 24 studies, Hunt et. al. showed that smokers were 1.38 times as likely to develop ccRCC (95% CI = 1.27-1.50). Male smokers had a higher risk of ccRCC, with a relative risk of 1.54 (95% CI = 1.42-1.68), while the relative risk for female smokers was 1.22 (95% CI = 1.09-1.36).
Obesity is an additional risk factor for ccRCC. Bergstrom et. al. conducted a meta-analysis of 24 studies, finding an increased risk of ccRCC for men in all but two studies, and in all but one study for women. A quantitative analysis of the same study set found a relative risk of 1.07 (95% CI = 1.05-1.09) for every unit of BMI gained, for both men and women.
The final risk factor of note is hypertension, defined as above-average blood pressure (~120mmHg). A 2008 study of the EPIC cohort by Weikert et. al. showed a relative risk of 1.61 for patients between 120mmHg and 139mmHg (95% CI = 0.81-3.21), a relative risk of 1.42 for patients between 140mmHg and 159mmHg(95% CI = 0.69-2.94), and a relative risk of 2.42 for patients above 160mmHg(95% CI = 1.13-5.19).
SDH and PPGLs
SDH mutations are strongly linked to paragangliomas. In a 2002-2014 retrospective analysis of 264 patients at the Ruijin Hospital, Shanghai Jiao Tong School of Medicine, 66.7% of patients with SDHB underexpressed developed progressive paragangliomas or pheochromocytomas, compared to 15.7% without normal SDHB levels (P=0.001). Furthermore, SDHB underexpressed patients had lower overall survival. In a prospective analysis of 217 patients from 2015 to 2020, the same study found that 18.8% of patients with SDHB underexpressed had progressive tumors, compared to 3.35% without SDHB underexpression (Su et. al., 2023).
66.7% of patients with SDHB underexpressed developed progressive paragangliomas or pheochromocytomas, compared to 15.7% with normal SDHB levels
The location of the SDH mutation (SDHA, SDHB, SDHC, SDHD) is somewhat predictive of the severity and location of disease. A 2004 analysis of 2 pheochromocytoma registries from Germany and Poland found that, among the 12% of patients with SDH mutations, SDHD mutation carriers were more likely to have multifocal head and neck paragangliomas (P<0.001), while SDHB mutation carriers developed malignant disease more frequently (P<0.001). In particular, eleven SDHB mutation carriers had malignant pheochromocytomas or paragangliomas, while no SDHD mutation carriers had malignant disease (Neumann et. al., 2004).
In a more recent 2021 genomic survey of 950 pheochromocytoma/paraganglioma patients from the UK, the Netherlands, and Germany, Bayley et. al. showed that truncating mutations - i.e. mutations that lead to shortening of the coding sequence - in both SDHB and SDHD were overrepresented among clinical patients and were associated with lower patient survival rates.
Overall, among the 403 unique germline mutations identified as of 2015, 19% were present in malignant tumors, and of these mutations, the vast majority (76%) occurred in SDHB, while 19% occurred in SDHD, and 5% in SDHC (Evenepoel et. al., 2015).
Environmental factors and PPGLs:
Due to its nature as a primarily germline disease, little research exists as to environmental factors influencing its development or progression. So far, only one environmental risk factor for PPGL is recognized, which is chronic high-altitude hypoxia. A 2003 study of 58 patients from the United States and the Netherlands by Astrom et. al. revealed that patients with single tumors lived at lower average elevations than those with multiple tumors (P<0.012), and that patients who developed pheochromocytomas lived at higher altitudes for longer (P<0.026). Furthermore, populations in the Netherlands, where the average person lives at a height of 2m (P~0), had a higher rate of germline SDH mutations, while populations in the United States, with a population-weighted average elevation of 260m (P~0), had lower rates of germline SDH mutations. This suggests that lower altitudes decreased the penetrance of germline mutations, reducing the selective pressure against them and increasing their prevalence.
This suggests that lower altitudes decreased the penetrance of germline mutations, reducing the selective pressure against them and increasing their prevalence.
Conclusion:
Succinate dehydrogenase represents a high-impact genomic factor in the development and progression of several cancers. Of particular interest is the role of SDH in ccRCC, in which the gene was previously assumed to only affect a small subset of the patient population but has very recently been found to be commonly suppressed. However, additional work is needed to determine the effects of increased SDH suppression on patient outcomes. The relationship between SDH and PPGL is much more defined, though more work is needed to explain and define the difference in patient outcomes caused by mutations to different subunits of SDH. It is also crucial to identify and study additional environmental factors affecting PPGL, as there is little data on correlations between race, income, or healthcare access and PPGL incidence. Altitude, the most-studied environmental factor, still demands additional research to clarify the exact roles of altitude vs. time spent at altitude.
References
- Aggarwal, R. K., Luchtel, R. A., Machha, V., Tischer, A., Zou, Y., Pradhan, K., Ashai, N., Ramachandra, N., Albanese, J. M., Yang, J.-I., Wang, X., Aluri, S., Gordon, S., Aboumohamed, A., Gartrell, B. A., Hafizi, S., Pullman, J., & Shenoy, N. (2021). Functional succinate dehydrogenase deficiency is a common adverse feature of clear cell renal cancer. Proceedings of the National Academy of Sciences, 118(39). https://doi.org/10.1073/pnas.2106947118
- Al Subhi, A. R., Boyle, V., & Elston, M. S. (2022). Systematic review: Incidence of pheochromocytoma and paraganglioma over 70 years. Journal of the Endocrine Society, 6(9). https://doi.org/10.1210/jendso/bvac105
- Aygun, N. (2020). Pheochromocytoma and paraganglioma: From epidemiology to clinical findings. SiSli Etfal Hastanesi Tip Bulteni / the Medical Bulletin of Sisli Hospital. https://doi.org/10.14744/semb.2020.18794
- Bardella, C., Pollard, P. J., & Tomlinson, I. (2011). SDH mutations in cancer. Biochimica Et Biophysica Acta (BBA) - Bioenergetics, 1807(11), 1432-1443. https://doi.org/10.1016/j.bbabio.2011.07.003
- Bayley, J. P., Bausch, B., Jansen, J. C., Hensen, E. F., van der Tuin, K., Corssmit, E. P., Devilee, P., & Neumann, H. P. (2021). SDHB variant type impacts phenotype and malignancy in pheochromocytoma-paraganglioma. Journal of Medical Genetics, 60(1), 25-32. https://doi.org/10.1136/jmedgenet-2020-107656
- Bayley, J.-P., Devilee, P., & Taschner, P. E. (2005). The SDH mutation database: An online resource for succinate dehydrogenase sequence variants involved in pheochromocytoma, paraganglioma and mitochondrial complex II deficiency. BMC Medical Genetics, 6(1). https://doi.org/10.1186/1471-2350-6-39
- Evenepoel, L., Papathomas, T. G., Krol, N., Korpershoek, E., de Krijger, R. R., Persu, A., & Dinjens, W. N. (2015). Toward an improved definition of the genetic and tumor spectrum associated with SDH germ-line mutations. Genetics in Medicine, 17(8), 610-620. https://doi.org/10.1038/gim.2014.162
- Hsieh, J. J., Purdue, M. P., Signoretti, S., Swanton, C., Albiges, L., Schmidinger, M., Heng, D. Y., Larkin, J., & Ficarra, V. (2017). Renal cell carcinoma. Nature Reviews Disease Primers, 3(1). https://doi.org/10.1038/nrdp.2017.9
- Neumann, H. P. H. (2004). Distinct clinical features of paraganglioma syndromes associated with SDHB And SDHD Gene mutations. JAMA, 292(8), 943. https://doi.org/10.1001/jama.292.8.943
- Prasad, P., Kant, J. A., Wills, M., O'Leary, M., Lovvorn, H., & Yang, E. (2009). Loss of heterozygosity of succinate dehydrogenase B mutation by direct sequencing in synchronous paragangliomas. Cancer Genetics and Cytogenetics, 192(2), 82-85. https://doi.org/10.1016/j.cancergencyto.2009.04.009
- Schiavi, F., Demattè, S., Cecchini, M. E., Taschin, E., Bobisse, S., Del Piano, A., Donner, D., Barbareschi, M., Manera, V., Zovato, S., Erlic, Z., Savvoukidis, T., Barollo, S., Grego, F., Trabalzini, F., Amistà, P., Grandi, C., Branz, F., Marroni, F., . . . Opocher, G. (2012). The endemic paraganglioma syndrome type 1: Origin, spread, and clinical expression. The Journal of Clinical Endocrinology & Metabolism, 97(4), E637-E641. https://doi.org/10.1210/jc.2011-2597
- Skinner, D. G., Colvin, R. B., Vermillion, C. D., Pfister, R. C., & Leadbetter, W. F. (1971). Diagnosis and management of renal cell carcinomaA clinical and pathologic study of 309 cases. Cancer, 28(5), 1165-1177.
- Su, T., Yang, Y., Jiang, L., Xie, J., Zhong, X., Wu, L., Jiang, Y., Zhang, C., Zhou, W., Ye, L., Ning, G., & Wang, W. (2023). SDHB immunohistochemistry for prognosis of pheochromocytoma and paraganglioma: A retrospective and prospective analysis. Frontiers in Endocrinology, 14. https://doi.org/10.3389/fendo.2023.1121397
- Yang, J., Zhou, Y., Li, Y., Hu, W., Yuan, C., Chen, S., Ye, G., Chen, Y., Wu, Y., Liu, J., Wang, Y., Du, J., & Tong, X. (2022). Functional deficiency of succinate dehydrogenase promotes tumorigenesis and development of clear cell renal cell carcinoma through weakening of ferroptosis. Bioengineered, 13(4), 11187-11207. https://doi.org/10.1080/21655979.2022.2062537
About the Author
We are two junior-year students at Polytechnic School in Pasadena, California studying and researching biology.
Ennio enjoys mechanical and electrical engineering, reading science-fiction novels, and swimming. He writes in his free time and likes playing with his dog, Sebastien.
Jonathan is interested in music, athletic medicine, sports, and enjoys camping in nature. He loves to play guitar, write, and spend time with his family and friends.